
 Maybe the rats are not the source of the "Black Death" in the 14th century. (c)wikimedia.commons Maybe the rats are not the source of the "Black Death" in the 14th century. (c)wikimedia.commons I learned in school that in the 14. century the “Black Death” plague was caused by the bacterium Yersinia pestis which was transmitted by rat fleas. However, this may not be true. So yes, plague is caused by Yersinia pestis, but there are different infection ways: (I) from rat fleas to human, (II) from human ectoparasites (fleas and lice) to human and (III) from human to human by inhalation from infected droplets. But how you can find out many centuries later which infection way was the basis for the “Black Death”? The answer is: with mathematical models! Katharine R. Dean, et al. (PNAS 2018) created mathematical models for all three infection ways. So they were able to simulate how infection rates would develop over time for each type of infection. Then they fitted the simulation results to real outbreak data and showed that in many cases the “human ectoparasites to human” model fits best. Of course, it can still be that it was a mixture of different infection ways and that the main infection way differed from region to region. Nevertheless, it shows that the story which we learn in school, that the plague is caused by infected rats and rat fleas, is maybe too easy.
0 Kommentare
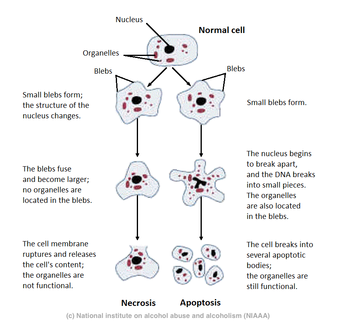 Your cells know two “dying” programs: apoptosis and necrosis. The latter results in swelling, ripping of the cell membrane, release of the cell content to the environment and therefore inflammation of the neighbour cells. In contrast, apoptosis is the self-induced and well-controlled suicide program of the cell which results in shrinking and fragmentation and doesn’t harm the neighbour cells. However, as always in life, the is not just black and white. Both processes have some similarities, especially in the beginning. Moreover, both can be triggered by similar toxic stimuli, and the “magnitude of the initial insult, rather than the type of the stimulus […] plays a critical role in the decision of the cell to undergo either apoptosis or necrosis.” The “decision” seems to be controlled by the intracellular ATP (energy) concentration, as apopotosis needs much more energy than necrosis. The hypothesis about the interplay between insult magnitude and intracellular ATP was tested by L. Formigli et al. (2000). They treted rat fibroblasts with different concentrations of Antimycin A, a toxin which blocks the mitochondrial respiratory chain and therefore leads to hypoxia (reduced oxygen content) and so to reduced ATP production. Indeed they were abel to show, that low Antimycin A concentrations, which result just in a small damage of the intracellular ATP storages, lead more to apoptosis, while high concentrations, which attack the ATP storages, lead to necrosis. Concentrations between resulted in mixed cell deaths: They showed apoptotic DNA fragmentation and degradation combined with necrotic cytoplasmatic swelling and membrane disruption. This mixed dying strategy L. Formigli et al. named “aponecrosis”. It seems like that cells which experience a toxic stimulus first try apoptosis, when there is still a certain amount of ATP left. However, if the ATP concentrations are depleted before the apoptosis process is finished, the cell switches to necrosis. So message of the day: (I) dying needs energy and (II) there are more than two ways to die. "Aponecrosis: morphological and biochemical exploration of a syncretic process of cell death sharing apoptosis and necrosis."
L. Formigli, et al. Journal of cellular physiology 182.1 (2000): 41-49. Evoked-response audiometry (or electric-response audiometry, ERA) is a collective term for techniques which record electrical activity response of the auditory pathway to auditory signals. These techniques allow conclusions about the hearing ability of the subject. According to the website corticalera.com, “the earliest report of relevance was that of Davis who identified the auditory cortical evoked response in 1939 although changes in the EEG evoked by a loud sound had been observed by Berger a decade earlier.” The first ERA technique was the cortical ERA (CERA) in which the cortical response is recorded from the vertex. Many tests had to be done for optimising the detection and analysis of the small bio-electronic signals. One of these tests is described in the paper of the day: “Validation of Evoked-Response Audiometry (Era) in Deaf Children” by Hallowed Davis (1966). It compares the ERA results with “old” testing methods for hearing ability which relied on behaviour signal to auditory signal. The measured ERA volume threshold for different auditory signals for different frequences differed from the voluntary thresholds (measured by behavioral response) just by 0.1dB. So no wonder that cortical ERA was in “widespread clinical use” just a handful of years later (in the 1970s). “Validation of Evoked-Response Audiometry (Era) in Deaf Children”
Hallowed Davis International audiology 5.2 (1966): 77-81 The Munchhausen syndrom is (simply speaking) when a person plays to be ill in order to get attention and sympathy. The Munchhausen syndrom by proxy is when e.g. parents manipulate medical history of their child simulate or exaggerates or induces health problems of their child by manipulating probes, lying about the medical history and giving damaging drugs. In 1977, the Munchhausen syndrom by proxy was quite unknown. Roy Meadow describes two cases of this form from child abuse and wonders that these cases “ [have] not been described in the medical literature.” The first case he describes is the little girl Kay. When she was 8 month old, urine infection was supposed the first time. Since then her life was full of antibiotics and “innumerable investigations and anaesthetic, surgical, and radiological procedures in three different [health care] centres.” Her mother which had had urinary-tract infections before, was a really caring and loving mother. However, later it was proven that she manipulated the urine probes of herself and the ones of her daughter. Maybe she did it because “she sometimes felt that her husband was more interested in the child than in her”. However, the brother of Kay was always healthy and no victim of the disordered psych of his mother. Fact is, as soon as the hospital controlled the contact between Kay and her mother, Kay was healthy again. So the story has a happy end. No happy end can be found in the second case of the Munchhausen syndrom by proxy which is described in Roy Meadow’s paper. Charles medical history began when he was 6 weeks old. He had attacks of vomiting and drowsiness. It was soon clear that his sodium concentration were too high but nobody was able to find out why this happened, especially as between the attacks he was normal and healthy. “By the age of 14 month it became clear that [the attacks] only happened at home” and that “the illness must be caused by sodium administration”. While he was in hospital no attacks occurred until the weekend when the mother visited her child. Unfortunately, this detection came too late. “During the period in which the local paediatrician, psychiatrist,and social services department were planning arrangements for the child”, Charles had to go to the hospital again and this time he died after he collapsed because of the extreme high sodium level in his blood. After this story I don’t feel like discussing Munchhausen sydrom and Munchhausen syndrom by proxy in a serious scientific manner. So let’s just sum up: we have to be aware that there is the possibility that the health status of a child is manipulated by its parents, even if the parents are friendly and lovely. That doesn’t mean that parents should not be asked for useful hints and that parents shouldn’t be allowed to visit their child in the hospital. Like Roy Meadow wrote: “We may teach, and I believe should teach, that mothers are always right; but at the same time we must recognise that when mothers are wrong they can be terribly wrong.” R.I.P. Charles "Munchausen syndrome by proxy: the hinterland of child abuse."
Roy Meadow The Lancet 310.8033 (1977): 343-345. 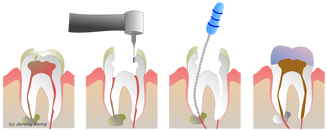 I am quite happy that I belong to the persons who had to google endodontic therapy. I feel sorry for every person who knows details about that because of their own experience. Every tooth contains nerves and blood vessels. They are coming through the root and are filling the pulp (the “hole” below the hard surface of the crown). Tooth damage (e.g. by cavity) can damage of the tooth or bacterial infection can lead to an infection of the nerves in the then unprotected pulp. In order to protect the tooth, the dentist removes all nerve tissue and the blood vessels (and other organic material). Desinfection secures that no bacterial infection will occur (again) in this tooth and then the holed tooth is filled with some material and protected by a crown. Herbert Schilder published a paper in 2006, in which he describes the problem of the three dimensional filling of the holed tooth. Filling material can be e.g. solid cores of gutta percha or silver which are connected to the tooth by cementing material. The problem is the complete sealing of the whole hole. The solid core needs to be adapted to the hole form and even then it is hard to guarantee that besides the main root canals all lateral accessory canals are sealed and protected from infection. Therefore, in addition to a solid gutta percha core, gutta percha (according to wikipedia: “a natural polymer prepared from latex from the percha (Palaquium gutta) tree”) can heated up. While gutta percha is heated up its get softer and helps to fill the gap between the the solid core and the tooth and so reduces the amount of cement which is needed. Lets hope we will never need that knowledge. "Filling root canals in three dimensions."
Herbert Schilder Journal of endodontics 32.4 (2006): 281-290. The todays paper reads a little bit like an ad for alternative medicine. It is about “the clinical practices and perceptions of professional herbalists providing patient care concurrently with conventional medical practice in Australia.” (Mavourneen Casey, et al. , 2007). Back then, in 2007, “a total of 1.9 million consultations for herbal medicine and naturopathy have been reported to occur annually in Australia.” I first thought that this isn’t much but this was due to a lack of my geographic knowledge. In the surprisingly small population of Australia of 23 million people (compared to Germany with 80million people), 1.9 million is around 8%. Herbal medicine comprises oral medication of strong pharmacologically active compounds. In a former "paper of the day" I wrote about the health supporting effect of the traditional Maori diet which included e.g. plants with cancer suppressing effects. Also “common pharmaceutical medications such as aspirin, morphine, codeine, atropine and digoxin were originally derived from herbal medicines.” So herbal medicine is interesting, especially its position to conventional medicine. Therefore, Casey et al. sent a postal survey “to all full members of the only national association of Western herbal medicine practitioners in Australia, the National Herbalists’ Association of Australia (NHAA).” The questions covered educational qualification and years of working experience of the herbalists as well as the methods/workflow of their therapy and the interaction with conventional medicine. Moreover, the herbalists were asked about their perceptions of their role in patient care, including medical diagnosis and the understanding of herbal therapy/pharmaceutical drug interactions. The results of the survey show a tight connection between herbal and conventional medicine. On the one hand, the number of herbalists with university qualifications increases which supports the trend of the integration of orthodox medical knowledge into herbal practices like blood test, lever function test and hormone profiles for treatment decision. On the other hand, the patients themselves tend to seek treatment in both medicines parallel. “Most patients who visit professional herbalists tend to seek care for chronic conditions, already have a medical diagnosis, and continue with concurrent conventional medical treatment.” This increases the risk of drug interactions. Therefore, in order to guarantee the safety of the patients, a study of the active compounds of the herbal medicine is important as well as a closer collaboration and cooperation between the medical communities. “An understanding of the ways in which herbalists practice and prescribe may be invaluable in the debate about the safety and efficacy of herbal medicines and may help the planning of reliable and valid research in the future.“ "An examination of the clinical practices and perceptions of professional herbalists providing patient care concurrently with conventional medical practice in Australia"
Mavourneen Casey, Jon Adams, and David Sibbritt Complementary therapies in medicine 16.4 (2008): 228-232 Maori were the first settler of New Zealand. Richard C. Cambie and Lynnette R. Ferguson published a paper in 2003 in which they discuss if the rise of diabetes, cancer and vascular related diseases in Maori people lately may be related to change in the diet. Were there any protective chemical constituents in the food plants of the traditional Maori diet which are now missing? In the survey they listed the chemical components of food plants which were part of the traditional Maori diet. Indeed they found a lot of different chemical constituents with anti-inflammatory, anti-cancer, anti-coagulation, anti-ulcer, anti-hepatoxin and anti-viral activity and positive effects on capillary walls and eye sight. This medical properties of the traditional Maori diet may suppressed diseases like diabetes, cancer and vascular related diseases but more details about the changed diet would be needed for a more detailed discussion. However, the survey shows the medical potential of some native plants in New Zealand. Potential functional foods in the traditional Maori diet.
Richard C. Cambie and Lynnette R. Ferguson Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis 523, 109-117 (2003) PMID: 12628508 |
IdeaI love to increase my general science knowledge by reading papers from different fields of science. Here I share some of them. Archiv
März 2018
Kategorien
Alle
|
 RSS-Feed
RSS-Feed
